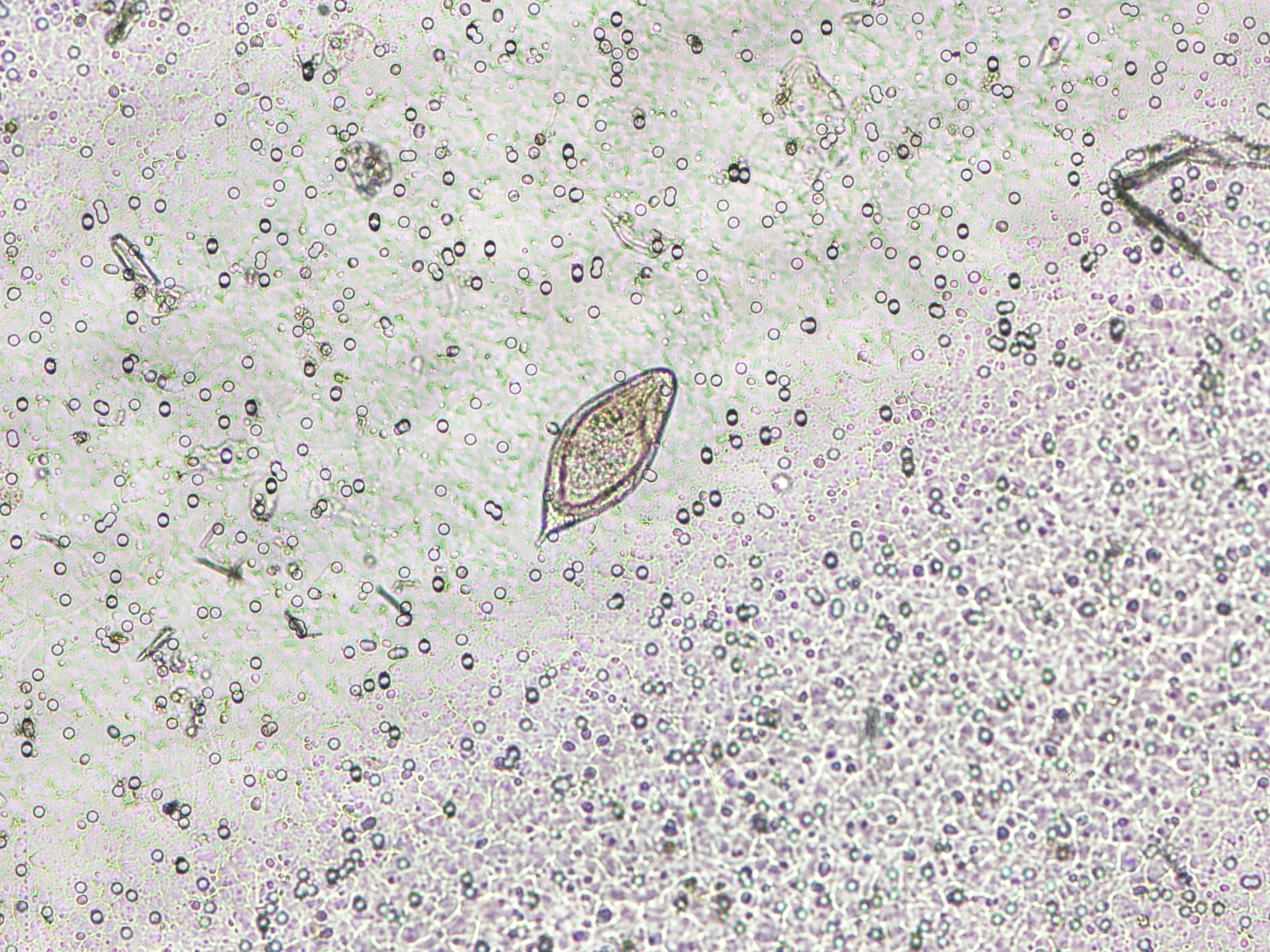
Answer: Ciliated epithelial cell. This cell likely arose from the caput epididymis, or possibly from an epididymal cyst of the male genitourinary tract that is lined by ciliated epithelium. The cilia continue to rhythmically beat even after the cells are detached from the rest of the epithelium (or even when the apical tuft containing the cilia has detached from the cell), and this may lead to a misdiagnosis of a parasitic infection. There are numerous reports of ciliated epithelial cells in respiratory epithelial cells being mistaken as trichomonads, free-living amebae,
Balantidium coli, and even the insect commensal,
Lophomonas. Less commonly, ciliated cells in male genitourinary specimens have been mistaken as parasites. Here is an older case report of a similar case that was mistaken for a parasite:
https://www.ncbi.nlm.nih.gov/pubmed/7495135
(email me if you want a copy of the article)
For future reference, here is a list of the sources of ciliated epithelium in the human body:
- Upper respiratory tract
- Fallopian tube and parts of the endometrium
- Ependymal cells that line the ventricles in the brain
- Caput epididymis/efferent ducts
- Any number of other locations where the epithelium has undergone a change called ciliary metaplasia (the epithelium converts from non-ciliated cells to ciliated cells)
Ciliated cells or detached ciliary tufts may be seen in specimens from any of these sources, and may be mistaken as parasites.
This was definitely a challenging case, and I loved seeing the great discussion that it generated! Huge kudos to Michigan Micro who pointed out the diagnostic features and led everyone away from a diagnosis of
Trichomonas vaginalis (which was the predominant answer for quite a while). These key features are:
Reason #1.
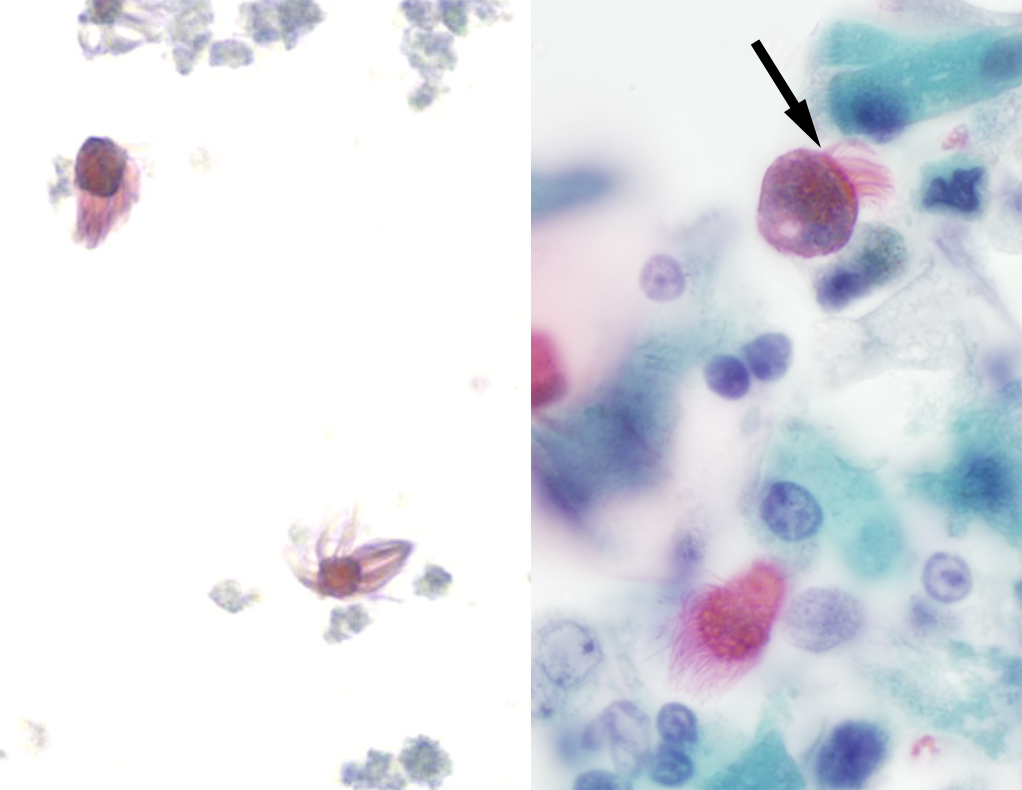
T. vaginalis doesn't have as many flagella as are seen in this case, and the flagella are more spaced out rather than grouped at one end. Compare the flagella of
Trichomonas (top photo below, arrow) to the dense mat of cilia (arrow) on respiratory epithelial cells (bottom image):
Shown in the bottom image are detached ciliary tufts (left) and degenerated ciliated epithelial cells (right; arrow points to the apical portion of the cell where the cilia arise).
The bottom right image looks a lot like the following still photos taken from this case:
Reason #2:
T. vaginalis has an undulating membrane, which is absent here (although it is hard to tell from the video).
Reason #3:
T. vaginalis has 'jerky' motility (see my previous case of the week for trichomonad motility
HERE - warning for obnoxious music)
Reason #4:
T. vaginalis is usually more rounded or pear-shaped, whereas this specimen is more elongated.
The last component to consider is size, which unfortunately was not provided with the case. However, here are sizes of similar-appearing objects for comparison:
- Trichomonas vaginalis trophozoites: 7-30 microns x 6-15 microns
- Detached ciliary tufts: 10-15 microns diameter
- Intact ciliated columnar epithelial cells: Generally 4 times longer than wide, so this would be approximately 40-60 microns long x 10-15 microns wide.
- Balantidium coli trophozoites: 40-100 microns in greatest dimension
































{kind=link}