Wow, there were a lot of great answers (and debate) on this case, and I found it interesting to see that many of the comments were also things that I considered when trying to identify this worm from just the available photographs. The specimen is obviously a long segment of tapeworm proglottids, and the two main worms in the differential are Taenia sp. and Diphllobothrium sp. The factors in favor of each are listed below:
In favor of Diphyllobothrium: long segment of proglottids, many of which are broader than they are long.
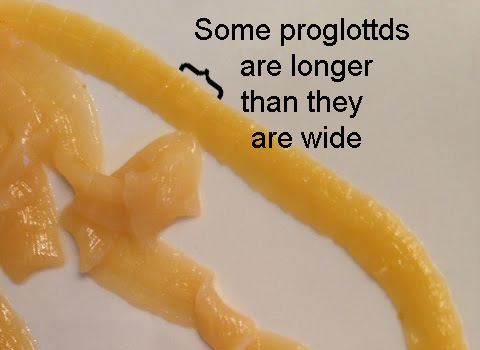
In favor of Taenia: Some proglottids are longer than they are wide (recall that immature Taenia proglottids are shorter), and there are no visible central uterine rosette structures as expected with Diphyllobothrium. In my experience, fresh Diphyllobothrium proglottids have a dark, prominent central uterine rosette which is notably lacking here (see cases 246 and 345) - and this case was certainly fresh! Therefore, I favored that this was Taenia rather than Diphyllobothrium.
So after counselling the patient against eating undercooked fish, pork and beef in the future, no further follow-up was thought to be necessary. There is a very small risk of cysticercosis in this patient (or family members) due to eggs that he was likely shedding in his stool, so he will also keep this in mind and monitor himself and his family for symptoms. Finally, there is still the unresolved question of what was causing the patient's eosinophilia. That clearly deserves further work-up and suggests infection with another worm (e.g. Strongyloides stercoralis), so additional testing and/or treatment is indicated.



No comments:
Post a Comment