Answer: Strongyloidiasis due to
Strongyloides stercoralis
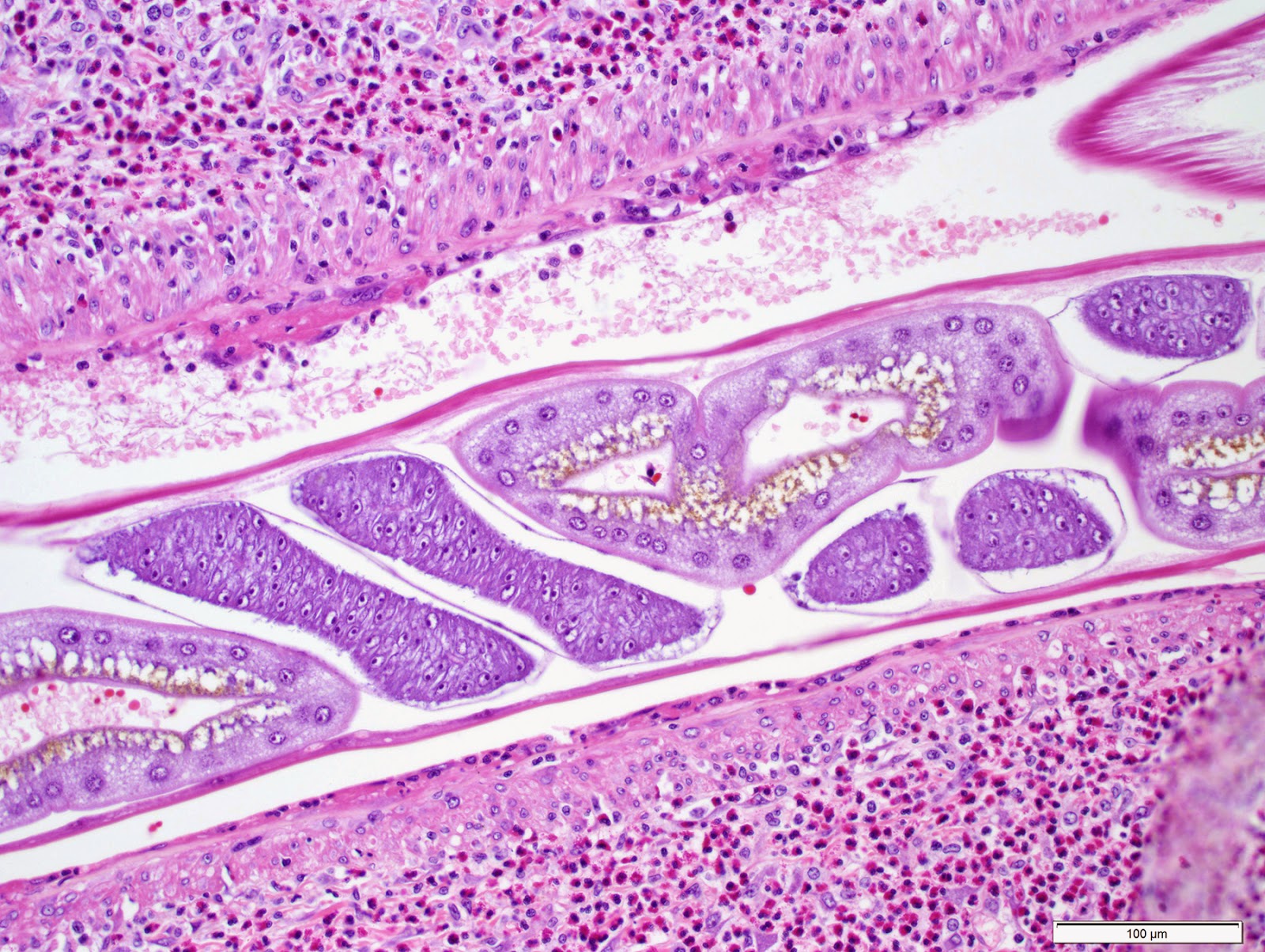
As with most biopsies of
S. stercoralis, all 3 parasite forms can be seen: the adult female, larvae and eggs:
Note that the eggs resemble those of hookworm. However, unlike human hookworm infection, eggs are never seen in the stool since they hatch to release rhabditiform larvae within the intestine. I like how you can see different stages of cell division within the eggs in this case:
As mentioned by Arthur, this diagnosis fits with the patient's clinical presentation. He states "I would guess that it (the infection) was benign until immunosuppressive chemotherapy began to treat the cancer, at which point a hyperinfective syndrome developed due to the opportunistic and autoinfective nature of this worm. The respiratory failure is likely due to the damage the worms do during the pulmonary stages of the life cycle, and sepsis is well documented in hyperinfective strongyloidiasis due to the filariform larvae penetrating the mucosa to reach the circulatory system, dragging coliform bacteria into the blood stream."
Of note, we take advantage of the propensity for larvae to drag bacteria with them when we use the stool agar culture method to detect
Strongyloides stercoralis and other nematodes
. When present in a stool specimen, the larvae migrate into the surrounding agar, dragging bacteria with them. The bacteria grow in the tracks, thus producing visible evidence of the larval migration. The agar culture method is the most sensitive means for detecting
Strongyloides stercoralis in stool (slightly more sensitive than the older Baermann method - and nicer to perform from a laboratory standpoint because there is no stool in an open container on the benchtop!) You can see some images of
S. stercoralis on culture plates in
Case of the Week 137, and most recently, by the impressive case donated by Lee (
Case of the Week 337). Note that you don't need a special type of agar to see the tracks left by
Strongyloides - anything that supports bacterial growth will work. The risk comes from accidental exposure to laboratory techs when they handle the plates with bare hands since
Strongyloides stercoralis and hookworm larvae can penetrate intact skin. When we perform the agar culture test in the parasitology lab at my institution, we always tape up the plates and put them in a transparent plastic bag for incubation at room temperature.