
Monday, December 24, 2012
Sunday, December 23, 2012
Answer to Case 238
Answer: Pediculus humanus
As pointed out by Hans, P. humanus has 2 ecotypes, which are referred to as head lice and body lice. Although they are very similar and have overlapping body features, they differ by only a single gene and can successfully interbreed to produce fertile off-spring. Here is an interesting review on human head and body lice which covers the taxonomy in greater detail:
Veracx and Raoult. Biology and genetics of human head and body lice. Trends in Parasitology, December 2012, Vol. 28, No. 12.
Enjoy, and Happy 2013!
As pointed out by Hans, P. humanus has 2 ecotypes, which are referred to as head lice and body lice. Although they are very similar and have overlapping body features, they differ by only a single gene and can successfully interbreed to produce fertile off-spring. Here is an interesting review on human head and body lice which covers the taxonomy in greater detail:
Veracx and Raoult. Biology and genetics of human head and body lice. Trends in Parasitology, December 2012, Vol. 28, No. 12.
Enjoy, and Happy 2013!
Monday, December 17, 2012
Case of the Week 237
The following were seen in a concentrated stool wet preparation that had been stored in formalin for 6 months. They measure approximately 60 micrometers in greates dimension. Identification?



Sunday, December 16, 2012
Monday, December 10, 2012
Case of the week 236
The following were observed in skin scrapings from a 75 year old man with an itchy rash.
Identification?





Identification?
Unstained, 100 times original magnification

Unstained, 400 times original magnification

Unstained, 400 times original magnification (focal plane 1)

Unstained, 400 times original magnification (focal plane 2; note appendages)

Unstained, 400 times original magnification (focal plane 3)

Sunday, December 9, 2012
Answer to Case 236
Answer: Scabies mites (Sarcoptes scabiei)
Note that the specimen shown appears to have 6 legs, indicating that it is a nymph. Like all other acari (inc. ticks and mites), the adult will have 8 legs.
I like this case in that you can clearly see the features of the developing nymph inside the egg.
You can also appreciate the short stumpy legs terminating in spines.

Note that the specimen shown appears to have 6 legs, indicating that it is a nymph. Like all other acari (inc. ticks and mites), the adult will have 8 legs.
I like this case in that you can clearly see the features of the developing nymph inside the egg.
You can also appreciate the short stumpy legs terminating in spines.

Monday, December 3, 2012
Case of the Week 235
This week's case is a bit challenging.
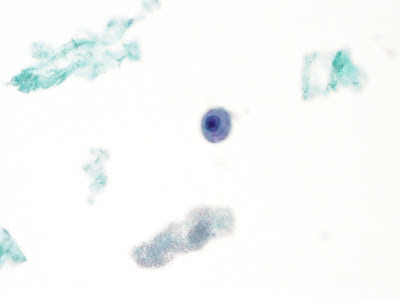
The following objects were seen in a Papanicolaou-stained endocervical preparation by the screening cytologist and brought to the microbiology lab for identification. They measure approximately 8-10 micrometers in diameter. The woman is asymptomatic. (shown at 1000 times original magnification)



Identification?
The following objects were seen in a Papanicolaou-stained endocervical preparation by the screening cytologist and brought to the microbiology lab for identification. They measure approximately 8-10 micrometers in diameter. The woman is asymptomatic. (shown at 1000 times original magnification)




Identification?
Sunday, December 2, 2012
Answer to Case 235
Answer: Presumed amebae; either non-pathogenic amebae from GI contamination or possible free-living organisms.
I posted this case because it was challenging for me as well and I wanted to see what the others had to say. Of the comments I received, the votes were as follows:
Amebae, (various types) - 8 votes
Chlamydia-infected epithelial cells - 1 vote
White blood cell, NOS - 1 vote
Trichomonas vaginalis - 2 votes
I was happy to see that the consensus supported my initial diagnosis. The features that I feel support the identification of ameba include the small size (< 10 microns in diameter), small nucleus (smaller than would be expected for an epithelial cell or macrophage) with large nucleolus/karyosome, and what appears to be phagocytosed material in the cytoplasm:

Thank you for writing in with your comments!
I posted this case because it was challenging for me as well and I wanted to see what the others had to say. Of the comments I received, the votes were as follows:
Amebae, (various types) - 8 votes
Chlamydia-infected epithelial cells - 1 vote
White blood cell, NOS - 1 vote
Trichomonas vaginalis - 2 votes
I was happy to see that the consensus supported my initial diagnosis. The features that I feel support the identification of ameba include the small size (< 10 microns in diameter), small nucleus (smaller than would be expected for an epithelial cell or macrophage) with large nucleolus/karyosome, and what appears to be phagocytosed material in the cytoplasm:

Thank you for writing in with your comments!
Sunday, November 25, 2012
Case of the Week 234
A large "worm" (several cm in length) was passed in the stool of a 4-year old boy. Unfortunately, rather than being submitted intact to the microbiology laboratory, it was sent to surgical pathology where slides containing serial cross-sections were produced. Below are representative H&E images taken at 40 and 100 times original magnification:







Identification?







Identification?
Saturday, November 24, 2012
Answer to Case 234
Answer: Earthworm
Given the larger size of this worm, Ascaris lumbricoides would be at the top of my differential. However, note that this worm does not contain a thick acellular cuticle and a layer of tall circumferential muscle cells as would be expected for this nematode. Instead, note that the outer cuticle is very thin and is underlain by tall epithelial cells containing mucin-producing cells. Below the epithelial layer are longitudinal and circumferential muscle cells, creating a thick muscular layer.

Finally, earthworms have a characteristic thickened band that is present near the anterior end of the worm called the clitellum. Fortunately we were able to capture a cross-section through the clitellum as shown below.

Of course, this worm could have been most easily identified if it had been submitted to the microbiology lab immediately, before it was sectioned, fixed, and embedded. I think Hans says it best with "Pathology, stay away from our worms!"
As to how this worm got into the boy's stool, I don't know if it was swallowed (would it survive the GI tract? Any volunteers to find out?) or ended up in the stool after it was passed.
Given the larger size of this worm, Ascaris lumbricoides would be at the top of my differential. However, note that this worm does not contain a thick acellular cuticle and a layer of tall circumferential muscle cells as would be expected for this nematode. Instead, note that the outer cuticle is very thin and is underlain by tall epithelial cells containing mucin-producing cells. Below the epithelial layer are longitudinal and circumferential muscle cells, creating a thick muscular layer.

Finally, earthworms have a characteristic thickened band that is present near the anterior end of the worm called the clitellum. Fortunately we were able to capture a cross-section through the clitellum as shown below.

As to how this worm got into the boy's stool, I don't know if it was swallowed (would it survive the GI tract? Any volunteers to find out?) or ended up in the stool after it was passed.
Tuesday, November 20, 2012
Case of the Week 233
A 67 year old contact lens wearer with eye pain was found to have a corneal ulcer. Corneal scrapings (unstained wet prep) revealed the following (CLICK ON IMAGES TO ENLARGE). The rounded structures measure approximately 15 micrometers in diameter.


Identification?
This case was generously donated by Dr. Julie Ribes.
Monday, November 19, 2012
Answer to 233
Answer: Cysts of Acanthamoeba sp.
These cysts have a very characteristic appearance, being uninucleat, usually between 10-25 µm in diameter, and possessing a wrinkled outer wall (exocyst) and hexagonal, polygonal, star-shaped, or spherical inner wall (endocyst).

These cysts have a very characteristic appearance, being uninucleat, usually between 10-25 µm in diameter, and possessing a wrinkled outer wall (exocyst) and hexagonal, polygonal, star-shaped, or spherical inner wall (endocyst).

Monday, November 12, 2012
Case of the Week 232
The following 17 mm x 9 mm skin ellipse was received in the Clinical Parasitology lab for identification. The container was marked "rule out retained tick mouth parts."

On closer examination, the center of the ellipse contained a dark irregular object:



Identification?
If you had received a phone call on how to best remove this object, what would have been your advice?

On closer examination, the center of the ellipse contained a dark irregular object:


Through careful dissection, I was finally able to extract the following:

Identification?
If you had received a phone call on how to best remove this object, what would have been your advice?
Sunday, November 11, 2012
Answer to 232
Answer: Retained tick mouthparts: toothed hypostome and part of the basis capituli. Unfortunately, it is not possible to definitively identify the genus of the tick from the parts available.
The answer to the second question is more interesting: If you had received a phone call on how to best remove this object, what would have been your advice?
Most of you correctly responded that the best way to remove a tick is by the use of forceps. The CDC has an excellent web page with instructions for removing ticks that you can access HERE. Excision is not necessary (!) unless the tick is not readily recognized (I've seen an engorged tick mistaken as an infarcted skin tag). In certain situations, retained mouthparts might also be difficult to remove without excising the surrounding skin, although the excised tissue does not need to be large.
In this case, the diagnosis (retained tick mouthparts) was only suspected which may explain why such a large excision was performed.
The answer to the second question is more interesting: If you had received a phone call on how to best remove this object, what would have been your advice?
Most of you correctly responded that the best way to remove a tick is by the use of forceps. The CDC has an excellent web page with instructions for removing ticks that you can access HERE. Excision is not necessary (!) unless the tick is not readily recognized (I've seen an engorged tick mistaken as an infarcted skin tag). In certain situations, retained mouthparts might also be difficult to remove without excising the surrounding skin, although the excised tissue does not need to be large.
In this case, the diagnosis (retained tick mouthparts) was only suspected which may explain why such a large excision was performed.
Monday, November 5, 2012
Case of the Week 231
A 40 year old woman retrieved a 'worm' from her nasal cavity and brought it to her primary care physician, who then submitted it to the laboratory for identification. The following images show the specimen that was received (pressed between 2 glass slides). (CLICK ON IMAGES TO ENLARGE)





.jpg)
40 times original magnification, unstained

100 times original magnification, unstained

200 times original magnification, unstained

400 times original magnification, unstained

400 times original magnification, unstained

400 times original magnification, unstained
.jpg)
Identification? How would you sign this case out?
Sunday, November 4, 2012
Answer to Case 231
Answer: Arthropod, not a human parasite. The spine-like structures seem to bit best with an adult insect. As Florida Fan said, "This seems like a 'flown in' case!"
Thank you for all of the comments on what the differential for "worm in nose" is. The main one is nasal myiasis, although the morphologic features would be very different than what is seen in this case. You can check out a previous case of myiasis involving the ear HERE.
Thank you for all of the comments on what the differential for "worm in nose" is. The main one is nasal myiasis, although the morphologic features would be very different than what is seen in this case. You can check out a previous case of myiasis involving the ear HERE.
Tuesday, October 30, 2012
Case of the Week 230
The following were seen in prostatic secretions from a man with chronic prostatis. Diagnosis?
Monday, October 29, 2012
Answer to Case 230
Answer: Flagellate protozoa, consistent with Trichomonas vaginalis or Pentatrichomonas hominis (a closely related GI commensal). The history of chronic prostatitis and location of the organism in prostatic secretions is most consistent with infection with the T. vaginalis, and this diagnosis was later confirmed by making permanently mounted and stained preparations of the organisms.
On wet prep, both organisms demonstrate a characteristic 'jerky' non-directional motility, which can be observed in the videos from this case. P. hominis trophozoites have similar morphology to those of T. vaginalis, but are typically smaller and the flagellum that forms the outer edge of the undulating membrane continues past the posterior end of the trophozoite as a free flagellum.
On wet prep, both organisms demonstrate a characteristic 'jerky' non-directional motility, which can be observed in the videos from this case. P. hominis trophozoites have similar morphology to those of T. vaginalis, but are typically smaller and the flagellum that forms the outer edge of the undulating membrane continues past the posterior end of the trophozoite as a free flagellum.
Monday, October 22, 2012
Case of the Week 229
A child presented with rapid onset of headache, confusion, and mental status changes after spending the weekend swimming in a warm fresh water lake. A lumbar puncture was performed and the following structures were seen in a Giemsa-stained cytospin preparation of CSF (CLICK ON IMAGES TO ENLARGE):
.jpg)
.jpg)
.jpg)
Unfortunately, the child quickly became obtunded and was declared brain dead within 24 hours of presentation. An autopsy was performed, which showed the following:




400 times original magnification
.jpg)
1000 times original magnification
.jpg)
.jpg)
Unfortunately, the child quickly became obtunded and was declared brain dead within 24 hours of presentation. An autopsy was performed, which showed the following:
40 times original magnification

200 times original magnification

400 times original magnification

1000 times original magnification

Diagnosis for this tragic case?
Sunday, October 21, 2012
Answer to Case 229
Answer: Primary Amoebic Meningoencephalitis (PAM) due to Naegleria fowleri. Naegleria fowleri trophozoites can be seen in both the CSF and the brain tissue. Note how the trophozoites originate from the leptomeninges and invade into surrounding brain tissue.

The trophozoites have a relatively small nucleus and large central karyosome, which allows them to be differentiated from human cells such as macrophages.

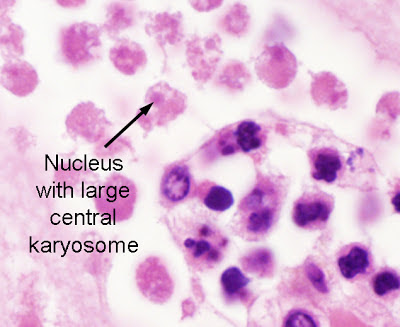
Similarly, the chromatin pattern with large karyosome differentiates the trophozoites of the free-living amoebae from those of Entamoeba histolytica (a rare cause of amebic CNS infection).
Although Naegleria fowleri has cyst, trophozoite, and flagellated forms in nature, it exists only in the trophozoite stage in humans, unlike the other free-living amebae (Balamuthia mandrillaris and Acanthamoeba spp.) which also have cyst forms in humans.
In this case, the characteristic trophozoites, lack of cyst forms, location in the meninges, and classic clinical history all support the diagnosis of PAM.

The trophozoites have a relatively small nucleus and large central karyosome, which allows them to be differentiated from human cells such as macrophages.


Similarly, the chromatin pattern with large karyosome differentiates the trophozoites of the free-living amoebae from those of Entamoeba histolytica (a rare cause of amebic CNS infection).
Although Naegleria fowleri has cyst, trophozoite, and flagellated forms in nature, it exists only in the trophozoite stage in humans, unlike the other free-living amebae (Balamuthia mandrillaris and Acanthamoeba spp.) which also have cyst forms in humans.
In this case, the characteristic trophozoites, lack of cyst forms, location in the meninges, and classic clinical history all support the diagnosis of PAM.
Tuesday, October 16, 2012
Case of the Week 228
The following objects were seen in a Pap-stained ThinPrep-preserved specimen of pleural fluid in a 50 year old male with chest pain, right fluid collection, and a lung mass.



+COW.jpg)
100x original magnification

200x original magnification

400x original magnification

400x original magnification
+COW.jpg)
Subscribe to:
Posts (Atom)


