
Monday, August 29, 2011
Case of the Week 174
The following were found in a vacant ski lodge which had not been occupied in several months. Identification? (CLICK ON IMAGE TO ENLARGE)

Sunday, August 28, 2011
Answer to Case 174
Answer: Bat bugs
Congratulations to all of my readers who got this right! I thought this might be a tricky case since bat bugs share many morphologic similarities with the ever-popular bed bugs. But most of you picked up on the subtle differences between the 2 arthropods.
As Blaine points out, "Given the length of the pronotal setae, they are bat bugs, Cimex sp. Cannot differentiate further without more geographic location (C. adjunctus in the east; C. pilosellus in the west)." Here are some web sites that highlight the important differences between these 2 bugs: BUGGUIDE and BADBEDBUGS
Congratulations to all of my readers who got this right! I thought this might be a tricky case since bat bugs share many morphologic similarities with the ever-popular bed bugs. But most of you picked up on the subtle differences between the 2 arthropods.
As Blaine points out, "Given the length of the pronotal setae, they are bat bugs, Cimex sp. Cannot differentiate further without more geographic location (C. adjunctus in the east; C. pilosellus in the west)." Here are some web sites that highlight the important differences between these 2 bugs: BUGGUIDE and BADBEDBUGS
Monday, August 22, 2011
Case of the Week 173
The following sections are from a skin biopsy of an itchy flank rash. Identification?
(H&E, 40x original magnification)

H&E, 400x original magnification

H&E, 400x original magnification

(H&E, 40x original magnification)

H&E, 400x original magnification

H&E, 400x original magnification

Sunday, August 21, 2011
Answer to Case 173
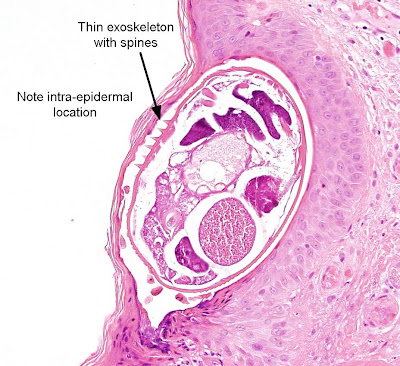
Answer: Scabies caused by the microscopic mite Sarcoptes scabiei.
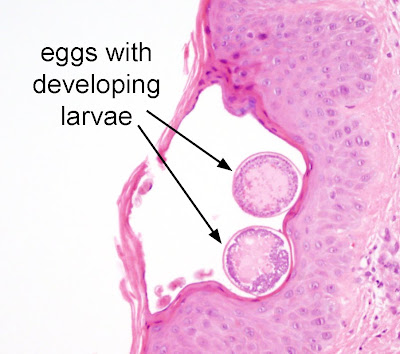
This mite burrows into the superficial layers of the epidermis and deposits eggs and fecal pellets (scybala). The diagnostic features of this case are:
1. The location within the epidermis
2. Size of mite and presence of toothlike spines on its thin exoskeleton (see below).
3. Adult and egg forms (below)
The best way to diagnose scapies is via skin scrapings (rather than biopsy). Skin scrapings can be obtained through which will produce mites with the best morphology. To obtain skin scrapings, mineral oil can be applied to the possible skin tracts followed by vigorous scraping with a sterile scalpel blade or glass slide. The material obtained should be placed on glass slides and examined for the presence of mites, larvae, and fecal pellets.
Anonymous and Neuronurse mentioned that this parasite resembles Gnathostoma spp, which also have spines on their external surface. However, Gnathostoma are uncommon in the epidermis (usually seen in subcutaneous tissue and viscera) and the spines are much smaller than those seen on the scabies mite. Gnathostoma also has different internal structures including large lateral cords. Good thought!
This mite burrows into the superficial layers of the epidermis and deposits eggs and fecal pellets (scybala). The diagnostic features of this case are:
1. The location within the epidermis
2. Size of mite and presence of toothlike spines on its thin exoskeleton (see below).
3. Adult and egg forms (below)


The best way to diagnose scapies is via skin scrapings (rather than biopsy). Skin scrapings can be obtained through which will produce mites with the best morphology. To obtain skin scrapings, mineral oil can be applied to the possible skin tracts followed by vigorous scraping with a sterile scalpel blade or glass slide. The material obtained should be placed on glass slides and examined for the presence of mites, larvae, and fecal pellets.
Anonymous and Neuronurse mentioned that this parasite resembles Gnathostoma spp, which also have spines on their external surface. However, Gnathostoma are uncommon in the epidermis (usually seen in subcutaneous tissue and viscera) and the spines are much smaller than those seen on the scabies mite. Gnathostoma also has different internal structures including large lateral cords. Good thought!
Monday, August 15, 2011
Case of the Week 172
A 35 year old immigrant from Sudan presents with fever. Images from a Giemsa-stained thin blood film are shown. Diagnosis? (CLICK ON IMAGES TO ENLARGE)









Sunday, August 14, 2011
Answer to Case 172
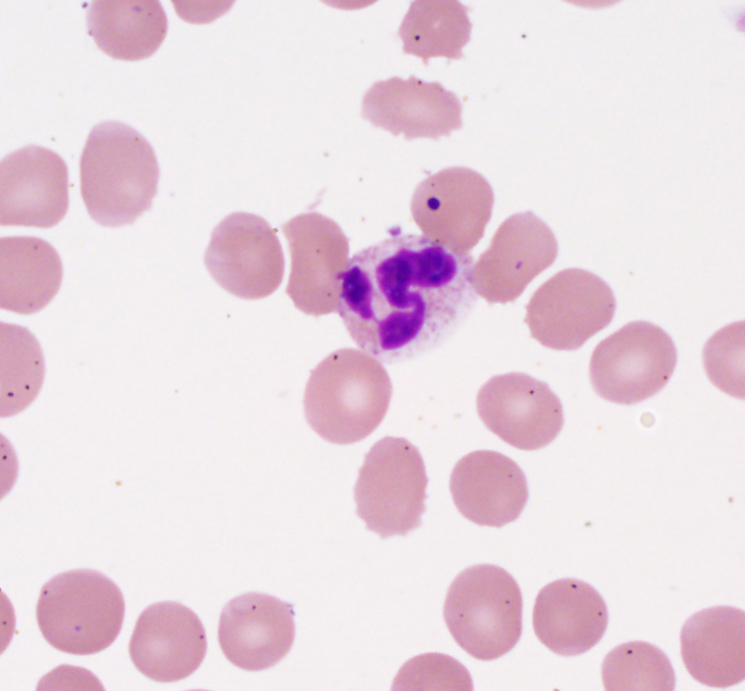
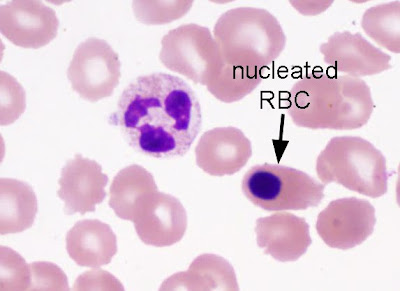
Answer: No blood parasites present; Howell-Jolly bodies, platelets, and a nucleated RBC present).
Great job everyone! Several respondents rightly raise the question of asplenia, given the Howell-Jolly bodies (nuclear remnants), nucleated RBCs, and RBC polymorphism with echinocytes (wrinkled RBCs with multiple spicules radiating from its circumference, resembling a sea urchin). These are common findings in a patient that does not have a functional spleen, since the spleen is responsible for removing RBCs that have not fully extruded their nucleus prior to entering the peripheral blood. We found out that this patient does NOT have a spleen which would explain the findings on this film.

This is a great example of a 'complicated' peripheral blood smear, in which
the exclusion of malaria or babesiosis can be quite difficult. The presence of Howell-Jolly does not exclude the presence of a blood parasite, so it is still important to examine these smears carefully. Anonymous raises the good point that PCR for malaria and babesiosis may be helpful when either of these infections are suspected. In this case, there was no evidence of blood parasites seen on thick and thin films, so we did not pursue PCR.
Other types of RBC "inclusions" include pappenheimer bodies (iron granules) and stain precipitate.
Finally, Anonymous mentions that the "tiny intraerythrocytic inclusions may be bacterial, like Bartonella. B. bacilliformis is the only one that's supposed to show up on peripheral smear, but no epidemiologic history to fit." This is a good thought, although as mentioned, it does not fit clinically. I would also expect the inclusions of B. bacilliformis to be more numerous and smaller than what is shown here.
Great job everyone! Several respondents rightly raise the question of asplenia, given the Howell-Jolly bodies (nuclear remnants), nucleated RBCs, and RBC polymorphism with echinocytes (wrinkled RBCs with multiple spicules radiating from its circumference, resembling a sea urchin). These are common findings in a patient that does not have a functional spleen, since the spleen is responsible for removing RBCs that have not fully extruded their nucleus prior to entering the peripheral blood. We found out that this patient does NOT have a spleen which would explain the findings on this film.


This is a great example of a 'complicated' peripheral blood smear, in which
the exclusion of malaria or babesiosis can be quite difficult. The presence of Howell-Jolly does not exclude the presence of a blood parasite, so it is still important to examine these smears carefully. Anonymous raises the good point that PCR for malaria and babesiosis may be helpful when either of these infections are suspected. In this case, there was no evidence of blood parasites seen on thick and thin films, so we did not pursue PCR.
Other types of RBC "inclusions" include pappenheimer bodies (iron granules) and stain precipitate.
Finally, Anonymous mentions that the "tiny intraerythrocytic inclusions may be bacterial, like Bartonella. B. bacilliformis is the only one that's supposed to show up on peripheral smear, but no epidemiologic history to fit." This is a good thought, although as mentioned, it does not fit clinically. I would also expect the inclusions of B. bacilliformis to be more numerous and smaller than what is shown here.
Sunday, August 7, 2011
Case of the Week 171
The following were seen on a peripheral blood thick film from a recent African immigrant. Identification? (CLICK ON IMAGES TO ENLARGE)










Saturday, August 6, 2011
Answer to Case 171
Answer: microfilaria of Wuchereria bancrofti
The first step in identifying this microfilaria is to recognize the presence of a poorly-staining sheath. The sheath is nicely demonstrated in images 3 and 4 of this case. This narrows your diagnosis down to one of the 3 following sheathed microfilariae:
1. Wuchereria bancrofti
2. Brugia spp. (sheath typically stains deep pink on Giemsa)
3. Loa loa
The next step is to look at the tail nuclei to differentiate the 3 microfilariae. Note in the image below that the nuclei do not extend to the tip of the tail. Therefore, this is consistent with W. bancrofti. (CLICK ON IMAGE TO ENLARGE)

I did not give you the size of the organism, but that is also a helpful differentiating feature.
Thank you everyone for your responses!
The first step in identifying this microfilaria is to recognize the presence of a poorly-staining sheath. The sheath is nicely demonstrated in images 3 and 4 of this case. This narrows your diagnosis down to one of the 3 following sheathed microfilariae:
1. Wuchereria bancrofti
2. Brugia spp. (sheath typically stains deep pink on Giemsa)
3. Loa loa
The next step is to look at the tail nuclei to differentiate the 3 microfilariae. Note in the image below that the nuclei do not extend to the tip of the tail. Therefore, this is consistent with W. bancrofti. (CLICK ON IMAGE TO ENLARGE)

I did not give you the size of the organism, but that is also a helpful differentiating feature.
Thank you everyone for your responses!
Tuesday, August 2, 2011
Case of the week 170
Multiple arthropods were submitted for identification to the Clinical Parasitology laboratory. No history was provided. A representative arthropod is shown below. How would you sign this case out?
Monday, August 1, 2011
Answer to Case 170
Answer: Not a human parasite; insect larva
The presence of multiple 'hairs' or spines on this larva is not consistent with fly larvae that cause human myiasis.
The presence of multiple 'hairs' or spines on this larva is not consistent with fly larvae that cause human myiasis.
Subscribe to:
Posts (Atom)


