Answer, Part I:
Trichinella spp. Although
Trichinella spiralis is the most common species to infect humans in the United States, it is generally not possible to speciate based on morphologic features. The exception is
Trichinella pseudospiralis whose larvae are not encapsulated compared to
T. spiralis,
T. nativa,
T. nelsoni,
T. britovi, and
T. murrelli which do have encapsulated larvae. These species are the predominant to infect humans.
Answer, Part II: What is the most common source of infection worldwide? Domestic pigs. What about in the United States? Wild game
According to a publication by the Centers for Disease Control and Prevention (Roy et al."Trichinellosis Surveillance --- United States, 1997--2001." Centers for Disease Control and Prevention), trichinellosis has been steadily decreasing in the United States due to tightened regulations on pig farming and pork processing. They state:
"Although trichinellosis was associated historically with eating
Trichinella-infected pork from domesticated sources, wild game meat was the most common source of infection during 1997--2001. During this 5-year period, 72 cases were reported to CDC. Of these, 31 (43%) cases were associated with eating wild game: 29 with bear meat, one with cougar meat, and one with wild boar meat. In comparison, only 12 (17%) cases were associated with eating commercial pork products, including four cases traced to a foreign source. Nine (13%) cases were associated with eating noncommercial pork from home-raised or direct-from-farm swine where U.S. commercial pork production industry standards and regulations do not apply."
The following is an excellent source of information on trichinellosis with beautiful photos: http://www.trichinella.org/index_synopsis.htm
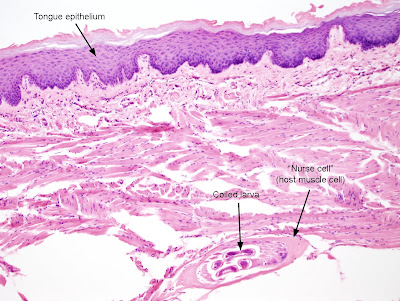
To make the diagnosis of trichinellosis on tissue section, one needs to recognize the classic appearance of the coiled larvae within tissue (typically skeletal muscle). Here is an image from this case that nicely demonstrates the larva, nurse cell (derived by the host) and stichosome (column of large rectangular cells).
(hematoxylin and eosin stained tissue section, 200x original magnification)

Note that in this case, the larva is located in the skeletal muscle of the tongue, right below the tongue's epithelium. (CLICK ON IMAGE TO ENLARGE)
(hematoxylin and eosin stained tissue section, 100x original magnification)
It is easiest to appreciate the coiled nature of the larvae by pressing non-fixed infected muscle between 2 slides and examining the tissue under the microscope. Here is an image from a previous case of the week that demonstrates a 'squash' prep:

Finally, for those of you non-pathologists who are having a hard time envisioning how a 3-dimensional coiled worm became a series of circles and ovals in tissue section, I've created the following diagram. The top image shows a coiled worm that is being cut along its longitudinal axis while making a slide. The bottom image shows how the worm would appear if you are only looking at the part that was cut and put on a slide.

Thanks to everyone who wrote in with the answer for this case!

























.jpg)

.jpg)