Wow, I can't believe we're up to case 70 already! I've really enjoyed the comments and suggestions from all of my readers.
Here are the answers to this week's case:
Identification?
Leishmaniasis. What is seen is the amastigote stage of this parasite. They live inside of macrophages, and range from 2-5 micrometers in greatest dimension. Therefore, the differential diagnosis includes other small intracellular yeasts such as
Histoplasma capsulatum. Also in the differential are
Toxoplasma gondii and
Trypanosoma cruzi (although both would be unusual in this site). The best way to tell Leishmania apart from yeasts and
T. gondii is to identify the rod shaped kinetoplast within each amastigote, in addition to the single nucleus. The arrows in the images point to what is most likely a kinetoplast. Note that it is very hard to see in a formalin-fixed, paraffin-embedded section! The best way to see the characteristic morphology is via a touch prep that is allowed to air dry and is then stained with giemsa (see below). Note that the kinetoplast is much more obvious.


These 2 Images from the CDC website:
http://www.dpd.cdc.gov/dpdx/HTML/ImageLibrary/G-L/Leishmaniasis/body_Leishmaniasis_il2.htmT. cruzi will also appear as clusters of intracellular amastigotes with kinetoplasts. However,
T. cruzi will infect any nucleated cell, and is typically found in smooth and cardiac muscle cells. In these cells, the amastigotes occupy a poorly defined pseudocyst, which is typically much larger than the small collection of
Leishmania amastigotes in infected macrophages.
A couple of other helpful hints:
1.
H. capsulatum has a pseudocapsule (seen as a clearing around each yeast)and no kinetoplast. (arrow head, below image - 1000 times original magnification, oil immersion)

2.
T. gondii is typically found in brain tissue (usually with necrosis in acute disease), and rarely, lymph nodes. The organisms have a classic arc shape on touch prep instead of the oval shape of the amastigote.
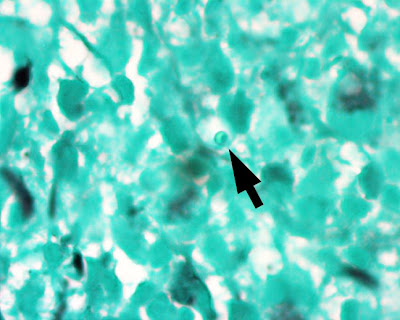
So what is the best way to differentiate
Leishmania from
H. capsulatum on formalin fixed tissue sections if you don't have an air-dried touch prep? A silver stain for fungi (e.g. GMS). The former is negative, while the latter is positive. The following is a silver stain performed on this case. The arrow points to a single amastigote, which is clearly NOT staining with GMS (1000 times original magnification, oil immersion).